
ResveratrolConsumer
avert online
consumer fraud
ResveratrolQuiz
test your knowledge
New E-Book
How the world got lost on
the road to an anti-aging pill
Subscribe to our newsletter to receive email notifications when new articles are posted.
October 26, 2015: by Bill Sardi
1000 AD: — “Here, eat this herb.”
1700 AD: — “That herb is an old wives’ tale; take this elixir.”
1900 AD: — “That elixir is quackery; take this pill.”
1960 AD: — “That pill doesn’t do any good; take this antibiotic.”
2015 AD: — “That antibiotic isn’t safe; take this herb.”
Modern medicine has reveled for over a decade in the most stupendous advancement in the history of cancer therapy, a drug discovery that added decades to the lives of patients with chronic myelogenous leukemia (CML) via a gene-targeted enzyme inhibitor. CML is the most common form of leukemia with around 5000 new cases diagnosed annually.
Patients who only had a few miserable years to live while they endured the side effects of interferon therapy can now live a normal lifespan and some no longer need to take medication at all, the true definition of a cure. Yet there is a dark side to this success in the war against cancer that is the topic of this report.
Pharmacology’s success was short-lived as latent treatment resistance was encountered after 4-5 years of use. This resulted in an expanded search for new molecules to reduce drug-resistant CML with slightly altered versions of the original medication.
Despite 3rd generation versions of the drug, the problem of treatment resistance persisted. So pharmacologists began a search for molecules that could be combined with the current medication and sensitize leukemic cells to die off. And that search has resulted in a horrific realization. That playing the current pharmaceutical game of developing patentable overpriced synthetic molecules to treat disease so as to produce billion-dollar blockbuster drugs not only results in the plundering of pooled health insurance funds but has also cost thousands of lives.
It is now recognized that a molecule found in nature could possibly have saved more lives with far less side effects at greatly reduced cost than the class of synthetic drugs in wide use today.
That lives have been needlessly lost by the insistence that only synthetic drugs are efficacious is a horror that is difficult to contemplate. Photographic evidence of this will be provided in this report.
In contrast to most newly introduced anti-cancer drugs that only prolong survival by a few months, Big Pharma glories in its one stupendous success in conquering cancer – the control of chronic lymphocytic leukemia (cancer of the blood) with a family of gene targeted enzyme inhibitors (tyrosine kinase inhibitors) that now achieve long-term cures and a near-normal lifespan despite some nagging but tolerable side effects. [Huffington Post 2015]
The wonder drug involved is imatinib, trade name Gleevec. A recent report says “although the treatment with imatinib achieves complete hematological remission in at least 95% of patients with chronic myelogenous leukemia (CML), total cytogenetic and molecular responses are relatively rare events… resistance to imatinib is a relatively common feature for patients with accelerated (disease).”
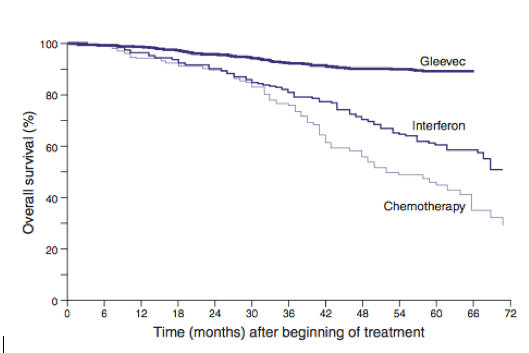
Overall Survival of patients with CML treated with imatinib (Gleevec), interferon or chemotherapy. Chemotherapy delivers only a minimum effect on survival compared with no treatment. [Lasker Foundation]
Researchers found a cancer gene called ABL, located on chromosome 9. Part of chromosome 9 fractures and translocates (transports) to chromosome 22 to bind with another gene to form what is known as the mutated Philadelphia chromosome. That other gene has been identified as the BCR gene. This ABL-BCR gene fusion is what fuels the cancer via over-activation of an enzyme called tyrosine kinase that causes white blood cells (lymphocytes) to grow and multiply incessantly. [Cancer Research UK 2012; Nature 1982] Therefore, tyrosine kinase inhibitors serve to treat and even cure this disease.
Imatinib, featured on the front cover of Time Magazine, was hailed as the new magic bullet against cancer, not just leukemia. It was what one cancer research organization called “the dawn of targeted treatments.”
Consider imatinib’s level of success:
This major advance in the war against cancer was dampened by unexpected drug resistance to imatinib and spawned many variations of inib” drugs (dasatinib, nilotinib, bosutinib, bafetinib, vemurafenib, erlotinib, gefitinib, crizotinib, ponatinib) with greater efficacy reported.
Nilotinib (Tasigna) is an “inib” family drug that was poised to replace imatinib (Gleevec) once its patent expired. A Bloomberg News report in 2012 said the strategy was to “portray Tasigna as the best treatment on the market, so good that there will be talk about it being a cure.” [FirstWord Pharma 2012]
Another “inib” family drug, bosutinib (Bosulif), a 3rd generation tyrosine kinase inhibitor, has been demonstrated to work when imatinib fails. [American Journal Health System Pharmacy 2015]
Ponatinib (Iclusig) has been described as the only tyrosine kinase inhibitor “with the capability to counter the highly resistance mutation in leukemic cells.” [Drugs Today 2013]
The FDA granted accelerated approval of ponatinib (Iclusig) in 2010 for newly diagnosed patients and had been approved for patients with treatment resistant disease in 2007. [National Cancer Institute 2013] But by October of 2013 a steady increase in the number of serious vascular occlusion (blood clotting) events and heart failure prompted the FDA to issue black box warnings. [Drugs 2014] This dampened the idea of ponatinib as the successor to imatinib.
The R&D challenge that still remains is how to overcome imatinib resistance that arises in about 15% of patients within 5 years of diagnosis. Drug resistant CML has been tracked down to a stubborn gene mutation identified as T3151. [Japanese Journal Clinical Oncology 2015]
Another goal is to increase the number of patients who can cease taking drugs altogether because they have undetectable leukemia. Around 30-40% of CML patients remain free of their disease for up to 2 years following cessation of imatinib. [Neoplasma 2015; British Journal Haematology 2014]
While imatinib’s success in prolonging life is measured in decades versus earlier cancer drugs that only added a few months to survival, it is very costly. Its price rose from ~$30,000/year in 2001 to $76,000 in 2015. It only costs $200 to manufacture a year’s supply of this miracle drug. [Huffington Post 2015; WBUR Sept 25, 2015]
One 400-milligram imatinib pill a day is required for effective treatment. That amounts to $208 per pill/day (costs 46-cents to manufacture). Imatinib generated $4.7 billion in sales annually. [FirstWord Pharma 2012] It is estimated there are ~60,000 patients who take ematinib daily.
Now that the patent on imatinib has expired, the drug company that owns the patent on imatinib bought off a competitor and delayed the entry of a generic version that would save a half billion dollars or more. [Wall Street Journal 2014]
Over time it became clear that continued development and introduction of newly fashioned “inib” drugs was not going to remedy the problem of drug resistance. Big Pharma needed to go in another direction — how to make leukemia cells more sensitive and less resistant to “inib” drug treatment.
A key finding is that resveratrol strongly addresses imatinib resistant leukemia cells. While imatinib kills off imatinib-sensitive leukemic cells it does not inhibit drug-resistant cells. Resveratrol doubled the sensitivity of leukemic blood cells in imatinib-sensitive cells, so resveratrol is not just to be confined to treatment of drug resistant cells. Researchers characterized resveratrol’s ability to quell leukemia as having “remarkable efficiency to induce cell death in treatment resistant cells.” [FASEB Journal 2008]
In 2010 a landmark report convincingly showed that resveratrol induces programmed cell death in both drug-sensitive and drug-resistant CML cells. [Cancer Research 2010]
Resveratrol is that widely extolled red wine molecule that has been widely researched but largely confined to animal studies rather than human use. A researcher who dared to bring resveratrol to the fore to prevent mortal heart attacks was falsely accused of scientific fraud and the stress of it led to his early death and threats to the nutraceutical company that offered such a pill. [Resveratrol News 2015]
Resveratrol has been documented to independently succumb chronic myeloid leukemic cells. There is scientific discussion as to whether resveratrol kills off leukemic cells via its toxic effects or its ability to non-toxically induce cell death via a biological process called apoptosis (programmed cell death). [Biochemical Pharmacology 2004]
In one study imatinib induced 50-60% of leukemic cells to die off via apoptosis (programmed cell death). [Cancer Biology & Therapy 2007] For comparison, resveratrol alone induced apoptosis in 43% to 59% of in both drug sensitive and drug-resistant forms of myeloid leukemia cells. [Anticancer Research 2012]
There is compelling evidence that resveratrol induces programmed cell death (apoptosis) in many types of cancer cells tested in a lab dish. [Cancer Research 2010] For example, resveratrol-induced apoptosis of human chronic myeloid (K562) and acute lymphoblastic (HSB-2) leukemia cells
Over a decade ago researchers reported that resveratrol is a promising molecule for chronic leukemia by virtue of its ability to inhibit treatment resistance and induce apoptosis (programmed cell death) as well as inhibit anti-apoptotic proteins. [British Journal Haematology 2002]
Both resveratrol and quercetin, another natural molecule found in red apple peel and red onion, block growth of chronic lymphocytic leukemia cells in a lab dish via their ability to induce programmed cell death (apoptosis) and slow down the cell renewal cycle, thus giving more time for genetic mutations to be repaired. [Hematology 2013]
Resveratrol’s biological mechanisms were more clearly documented over time. By virtue of its ability to activate a cell energy-sensing molecule called AMPK, resveratrol inhibits the enzyme (tyrosine kinase) that drives the growth of leukemic cells. [Oncotarget 2011]
In a newly published study, compelling photographic images are presented below which show that resveratrol alone, not in combination with imatinib, kills of leukemic (K5562) cells even more effectively than imatinib. [Genetics & Molecular Research 2015]

The authors of this landmark study write: “the combination of imatinib and resveratrol may be a more effective strategy for human CML therapy. The combination of imatinib and resveratrol represents a paradigm shift in cancer drug development. This may result in a new generation of specific targeted therapies for the numerous malignant conditions for which no efficient drug therapy is currently available.” [Genetics & Molecular Research 2015] Yet their data and blood slides reveal resveratrol is also very effective when used alone. Researchers can’t make their lips say what has now become clear – resveratrol is superior to the entire family of “inib” drugs.
There is nothing keeping physicians from combining resveratrol with “inib” drug therapy among terminal patients with progressive leukemia, to be used on a compassionate care basis. FDA approval is not necessary. Resveratrol is a widely available dietary supplement that has not produced notable serious side effects in the past 10 years over a wide range of doses. Why all the foot dragging?
In the 1990s pharmacologists had screened hundreds of molecules for one that would inhibit tyrosine kinase. They must have bumped into resveratrol in that screening. It has been known since 1993 that resveratrol strongly inhibits tyrosine kinase. [Journal Natural Products 1993]
Why had resveratrol remained in the research closet so long?
An authoritative report says: “Surprisingly, despite promising in vitro (lab dish) and in vivo (lab animal) effects, resveratrol has not yet been analyzed as a potential therapeutic agent for the treatment of chronic myeloid leukemia.” [FASEB Journal 2008]
Don’t tell us that all along resveratrol has been a more viable alternative to imatinib. Don’t tell us that thousands of CML patients met their premature death while pharmaceutical companies schemed how to profiteer ahead of providing a cure. This is a horror story, a story of greed over cure.
The concentration of resveratrol required to inhibit the growth of leukemia cells has been determined and is achievable via oral consumption.
In various lab dish studies resveratrol has been demonstrated to be effective in killing off leukemic cells at a concentration ranging from 25-160 micromole per milliliter. [International Journal Clinical Experimental Pathology 2010; FASEB Journal 2008; Biochemical Pharmacology 2004; Anticancer Research 2012]
One study shows that every 25 milligrams of oral resveratrol equates with a 2-micromole rise in blood levels in humans. To achieve a 25- micromole/milliliter blood concentration about 250-325 milligrams of resveratrol would be required for a 160-lb (70 kilogram) person. This would make a good starting dose for human clinical use.
Excessive resveratrol dosing can produce reversible side effects such as Achilles heel tendonitis, headaches, anxiety reactions, racing heart and flu-like symptoms. Loose stool is sometimes experienced when using less pure forms of resveratrol derived from giant knotweed due to its emodin content. So mega-dosing is not recommended.
While leukemic patients may be dying needlessly modern pharmacology is predictably attempting to develop a synthetic analog (look-alike) of resveratrol that can be patented to combine with “inib” drugs. [International Journal Oncology 2007; Molecular Pharmacology 2015] Big Pharma must profiteer before it cures.
The bogus claim that resveratrol is not biologically available will aired as the reason to develop synthetic resveratrol analogs. Resveratrol is bound to detoxification molecules as it passes through the liver in the blood circulation thus rendering it temporarily unavailable. However, these liver metabolites (resveratrol conjugated with sulfate or glucuronate) are biologically active in themselves and sometimes exceed the activity of unbound (free) resveratrol. [Resveratrol News 2013]
Remarkably, resveratrol variably induces apoptosis depending upon the tissue and its biological state. In an experimental model of heart attack resveratrol inhibited programmed cell death (apoptosis), thus preserving more heart muscle cells and reducing scarring (fibrosis). [PLoS One 2010] Resveratrol also inhibits apoptosis (programmed cell death) in brain cells during periods of oxygen deprivation (stroke) but activates apoptosis to selectively kill off brain cancer cells. [Neuroscience Letters 2003; International Journal Clinical Experimental Medicine 2015; Journal Neurooncology 2007] As already presented in this report, in leukemic white blood cells resveratrol increases the die off (apoptosis) of leukemia white blood cells (lymphocytes). [Annals Hematology 2011]
What more do the drug companies know that they aren’t telling us about? For sure, they must know more about why some patients with chronic myelogenous leukemia don’t need to take tyrosine kinase inhibitors any more. However, knowing how to effect a complete cure without the need to take drugs would be counterproductive to the drug industry.
The process that leads to a full cure surely must have something to do with what is called epigenetic imprinting of genes involved in enzyme (tyrosine kinase) activation. [IntechOpen.com 2012]
It is known that a biological process called methylation, in this instance hypomethylation, causes chromosomal instability and translocations and deletions of genes and loss of genetic imprinting. Methylation is a biological process by which methyl groups are added to DNA.
Dietary factors can increase methylation and reduce over-activation of malignant genes. Vitamins like B12, B6, folic acid and betaine are methyl donors. Royal jelly from the bee hive is also a strong methylating agent. [EMBO Reports 2011] The lack of vitamins and other nutrients that control methylation can lead to the translocation of genes, as observed in acute myelogenous leukemia, that results in uncontrolled malignancies. [Leukemia 2014] Though there is some doubt that methylation controls translocation of the ABL-BCR gene involved in CML. [Leukemia 2014; Epigenetics In Cancer 2013]
Inherited aberrant metabolism of folate (vitamin B9) is associated with relapse among patients with CML. [Clinical Cancer Research 2004]
Over 15 years ago it was found that niacin (vitamin B3) induces programmed cell death (apoptosis) in human CML cells. [Bioscience Biotechnology Biochemistry 2000]
There is recent evidence that antioxidants such as vitamin E could be utilized with drugs like imatinib to reduce treatment resistance via inhibition of ABL-BCR gene mutations. [Leukemia 2014]
It has been reported that the combination of vitamin A + vitamin E induce programmed cell death (apoptosis) in leukemic cells. [Molecular Cell Biochemistry 2008] CML patients are known to have low vitamin E levels. [Journal Association Physicians India 2000]
The combination of vitamin K + vitamin C inhibits growth of human chronic myelogenous leukemia cells by about 60% in laboratory mice. [Biochemical Pharmacology 2006]
Low vitamin D levels have been linked to aggressiveness of leukemia. [Vitamin D Council; Hematology 2011]
Vitamin C alone has been demonstrated to overcome imatinib treatment resistance in leukemic cells. [Experimental Hematology 2004]
High stored iron levels (ferritin) are associated with higher incidence of relapse and poorer disease-free and overall survival among patients with acute myelogenous leukemia. [Leukemia Research 2015] Elevated iron levels inhibit programmed cell death (apoptosis). [Leukemia 2002] Removal of iron via blood letting or chelation (key-lay-shun) may improve survival of patients with leukemia. [Annals Hematology]
It is important to learn the cancer industry lives in a self-defined world of deceit. Recent criticism of the pharmaceutical industry includes the widely known fact that high-priced anti-cancer drugs often only add a few weeks to months to life. Yet even this reported marginal prolongation of survival often vanishes with assessment of overall survival rather than the narrower measure of cancer survival. Some new cancer therapies shrink tumors and appear to be advances but their mortal side effects often result in the more rapid demise of the patient from other causes, such as chemotherapy-induced heart failure or destruction of the immune system.
Furthermore, there is sleight of hand in quoting longer survival times with cancer therapies that are only achieved by earlier detection of cancer. Earlier diagnosis when tumors are smaller only appears to add to survival time but is meaningless as most patients are dying on the same calendar day.
The originator of imatinib foresees a future where molecular targets for each type of cancer are identified and synthetic drugs are then fashioned to treat each of them. [Nature Medicine 2009] But this approach suggests pre-cancer must be allowed to progress into full blown tumors, then diagnosed and treated, rather than development of a “drug” that would inhibit all forms of cancer, that is, prevent cancer. [Seminars Cancer Biology 2015] Resveratrol exhibits biological action against cancer that would require many different drugs to duplicate. [Nutrition Cancer 2012] The obvious preferable approach to cancer is to never let it get started rather than become totally dependent upon treatment. ©2015 Bill Sardi, Resveratrol News
Posted in Resveratrol
Add comments »